1.Introduction
Effective inventory management constitutes a critical pillar in the operational and clinical performance of hospitals. In resource-constrained settings—particularly low- and middle-income countries (LMICs)—public hospitals must reconcile the need for continuous availability of essential medicines and consumables with restricted budgets, erratic demand, and procedural procurement delays. The COVID-19 pandemic has magnified these pressures, exposing systemic fragilities in health supply chains and reinforcing the imperative for more adaptive, risk-sensitive inventory strategies.[1,2] In Vietnam and comparable LMIC contexts, these challenges are further intensified by evolving clinical profiles, seasonal epidemiological fluctuations, and inconsistent patient volumes—especially in pediatric tertiary hospitals, where supply–demand mismatches may lead to disproportionate clinical risks.
In such contexts, hospital pharmacies continue to rely on legacy inventory systems characterized by bulk purchasing, reactive restocking, and annual budgeting cycles. These systems typically operate in the absence of demand forecasting tools, clinical integration, or digital traceability. Local case studies have documented critical inefficiencies. For instance, a retrospective assessment at Thong Nhat Hospital in Ho Chi Minh City reported elevated rates of drug expiry and emergency procurement during peak periods, exacerbated by rigid restocking thresholds and lack of real-time consumption visibility.[3] Similarly, research at Kien Giang Provincial Hospital identified that fixed safety stock levels failed to accommodate clinical variation, prompting the application of EOQ modeling tailored to local operational rhythms.[4] Yet, such studies often focus on isolated interventions without examining the combined effects of classification systems, simulation models, and lean inventory strategies under operational constraints.
To address these issues, stratification-based inventory control models have gained traction. The ABC classification method—ranking items by annual consumption value—remains a foundational tool in hospital logistics, particularly in Asia and sub-Saharan Africa.[5,6] However, its one-dimensional focus on cost fails to account for temporal demand fluctuations, a limitation in clinical environments where usage is often episodic, seasonally variable, or emergent. The ABC–XYZ hybrid model has therefore gained prominence in high-acuity domains such as oncology, intensive care, and surgery, where both value and volatility require differentiated inventory policies.[7,8] This dual classification approach enables more nuanced risk segmentation, laying the groundwork for adaptive policy design across item categories.
Empirical findings support this shift. At an Indian tertiary cancer center, for example, application of ABC–XYZ analysis allowed managers to differentiate high-cost, low-variability (AX) items from low-cost, high-variability (CZ) items, thereby reducing both expiry losses and critical stock-outs.[7] Comparable results were observed in Malaysian type B pharmaceutical units, where stratified procurement thresholds expedited approvals and improved service continuity.[9] In Vietnam, the integration of ABC–VEN matrices has expanded this logic, incorporating clinical criticality alongside cost and variability in procurement decisions.[10] Nonetheless, most existing studies treat classification models as static decision-support tools rather than embedding them into active governance frameworks or validating them through real-world operational testing.
In parallel, simulation modeling and lean principles have gained recognition as valuable planning instruments. Lean Six Sigma initiatives in Peruvian pharmaceutical small and medium-sized enterprises (SMEs), for instance, demonstrated that combining ABC classification with Kanban and 5S improved stock turnover and minimized expirations.[11] Discrete-event simulation (DES) has also proven effective in stress-testing inventory policies under varied demand, supply, and delay scenarios, offering decision-makers a risk-free environment to explore reforms.[12,13]
The potential application of Just-in-Time (JIT) inventory strategies in healthcare has likewise received growing interest. Originally designed for manufacturing, JIT—when coupled with digital dashboards, predictive analytics, and dependable supplier performance—can reduce stockholding, accelerate turnover, and improve procurement responsiveness.[14,15] For instance, in a U.S. multi-hospital system, real-time connected dispensing technologies significantly reduced emergency procurement and backorders.[16] However, JIT adoption in LMICs remains limited due to rigid budget cycles, fragmented data infrastructure, and inconsistent vendor reliability.[17,18] More critically, existing studies rarely assess the feasibility of JIT implementation within public-sector hospital governance frameworks, particularly in pediatric contexts where stock-outs may delay urgent clinical interventions.
Taken together, ABC–XYZ classification, simulation modeling, and JIT strategies each offer unique operational advantages. Yet, the literature remains fragmented, with most studies exploring these approaches in isolation. Very few have examined their integrated use under real-world administrative and clinical constraints—especially in pediatric tertiary hospitals in LMICs, where inventory failure may have acute consequences.
Despite recent advancements, evidence remains scarce on how these tools perform collectively in practical LMIC hospital settings. Many studies overlook the systemic bottlenecks—such as procurement rigidity, data silos, and weak supplier performance—that complicate implementation and scale-up.[12,19] Moreover, pediatric hospitals are often underrepresented in empirical research, despite the high acuity, complex logistics, and heightened sensitivity to supply disruptions in these environments.[2,20] Thus, there is a pressing need for research that empirically tests the integration of classification, simulation, and lean inventory models under real-world constraints, with specific attention to scalability, institutional readiness, and clinical impact.
This study aims to address these gaps through a mixed-methods design combining retrospective inventory analysis, ABC–XYZ classification, discrete-event simulation (DES), and a targeted JIT pilot for high-risk clinical items. Conducted at a high-volume pediatric tertiary hospital in Vietnam, the research investigates whether a hybrid, risk-informed inventory strategy—anchored in both local realities and global best practices—can improve responsiveness, reduce wastage, and enhance continuity of care within the structural constraints of a public health system.[1,12,19,21] This staged, empirically validated integration of operational tools contributes distinctively to the literature on hospital inventory reform in LMICs. While prior research has evaluated ABC–XYZ, DES, or JIT in isolation, this study combines them within a unified, institutionally tested model—applied in a real-time hospital environment with verifiable governance, logistical, and fiscal limitations.
2.Methods
2.1Study design and scope
This study employed a multi-phase, mixed-methods design to evaluate the performance of hospital inventory management and assess the feasibility of transitioning to a JIT model. Conducted at Children’s Hospital 1, a high-volume tertiary pediatric facility in Ho Chi Minh City, Vietnam, the research covered the period from January 2019 to March 2025. The study combined retrospective data analysis, structured inventory classification, root cause exploration, simulation modeling, and prospective pilot validation. This design was chosen to balance empirical depth with contextual adaptability, ensuring that findings were operationally grounded and implementation-relevant.
2.2Data sources and collection
Quantitative data were retrospectively extracted from the hospital’s logistics and clinical information systems. These included:
- Monthly consumption and procurement records for over 1,200 high-tech medical supply items (2019–2024),
- Stock-out incidents, procurement cycle times, urgent purchase rates, and inventory turnover metrics,
- Clinical workload data (admissions, procedures, bed occupancy), used to contextualize supply demand.
In parallel, qualitative data were collected through 17 semi-structured interviews with stakeholders across procurement, supply chain, and clinical departments. Interviews focused on identifying systemic inefficiencies, procedural barriers, and gaps in coordination. The use of both retrospective records and real-time stakeholder input ensured triangulation and enhanced the validity of identified bottlenecks.
2.3Inventory classification framework
All medical supply items were classified using a dual-layer ABC–XYZ analysis:
- ABC analysis ranked items by annual consumption value, with Class A accounting for 70%–80% of total value, Class B for 15%–25%, and Class C for the remainder.
- XYZ analysis categorized items based on demand variability using coefficient of variation (CV) thresholds, with Class X indicating low variability, Y moderate, and Z high unpredictability.
The resulting ABC–XYZ matrix informed differentiated control strategies, risk segmentation, and selection criteria for simulation inputs and pilot targets. Items with high volatility (e.g., CZ, BZ) were flagged for additional analysis to understand their operational criticality and explore alternative stocking models beyond JIT.
2.4Root cause and gap analysis
To identify systemic bottlenecks, a root cause analysis was conducted using a triangulated approach. Quantitative trends in key performance indicators were combined with thematic coding of interview transcripts and cross-referenced with findings from internal audit reports (2020–2023). Bottlenecks were categorized according to their origin (process, data, structure, supplier) and mapped to their operational impact. This diagnostic step established the foundation for simulation modeling, ensuring that projected scenarios were grounded in empirically observed operational challenges rather than theoretical assumptions.
2.5Simulation modeling
A DES model was developed using Arena 16.1 to evaluate the JIT strategy under realistic constraints. Two scenarios were explored: (1) Baseline (2024), reflecting current workflows, and (2) JIT Scenario (2025), incorporating reduced cycle times (30 to 15 days), dynamic safety stocks, and VMI for high-priority items. Key input parameters are summarized in Table 1 to ensure transparency and reproducibility.
| Parameter | Value/Distribution | Source/Rationale |
|---|---|---|
| Arrival frequency | Poisson Distribution | Based on XYZ volatility |
| Demand volume | 29,246 surgeries; 840 cardiology cases | 2024 actual throughput |
| Cycle Time (Baseline vs. JIT) | 30 vs. 15 working days (Constant) | Administrative reform target |
| Supply delay | 13.3%–20.3% (Triangular Dist.) | Historical delivery lapses |
| Model Execution | 30-day warm-up; 100 replications | Steady-state validation (95% CI) |
| Safety Stock | Dynamic (Risk-adjusted) | Calibrated by ABC–XYZ matrix |
Simulation calibration was performed using historical operational data and refined through three iterative review cycles with logistics, procurement, and clinical stakeholders to ensure alignment with institutional processes. Model outputs were subsequently cross-validated against Q4/2024 performance benchmarks. Sensitivity analyses were conducted under alternative scenarios, including partial supplier compliance and conservative procurement cycle reductions (e.g., to 20 days)—to assess the robustness of projected outcomes. These analyses clarified structural constraints and strengthened the external validity of the proposed inventory reforms.
2.6Pilot validation
To validate simulation outputs, a pilot implementation of the JIT model was conducted in Q1/2025 within the Department of Cardiovascular Intervention. A total of 42 supply items, predominantly classified as AX and AY based on the ABC–XYZ matrix, were managed under JIT protocols. Core elements included:
- Integration of daily procedural logs with inventory systems,
- Barcode-enabled real-time tracking,
- Automated replenishment thresholds,
- VMI arrangements for selected high-volume items.
Performance during the pilot (Q1/2025) was benchmarked against Q1/2024, focusing on key indicators: stock-out incidents, urgent procurement rates, inventory days, holding costs, and procedure disruptions. In addition to quantitative metrics, structured interviews and rapid feedback sessions were conducted with clinical and logistics staff to assess operational feasibility, workload implications, and user acceptability.This dual focus on performance and perception provided a holistic assessment of both system-level impact and frontline experience, enabling a more grounded evaluation of scalability potential.
Figure 1 presents a structured overview of the study’s methodology, including the sequence of research phases, data sources, inventory classification logic, root cause diagnostics, simulation modeling setup, and pilot validation design. The visual framework illustrates the interdependencies across methods and clarifies how evidence from each phase informed the subsequent stage. Such iterative structuring reinforces methodological rigor and enhances the translational relevance of findings.
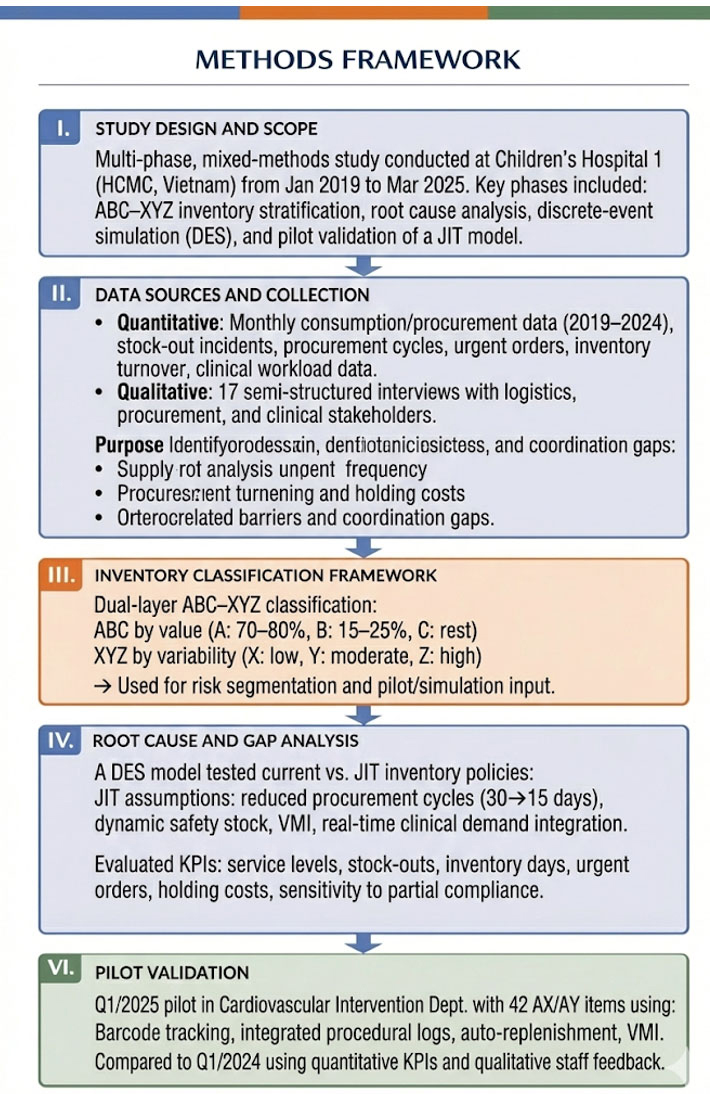
Figure 1.
Methods framework of the study
3.Results
3.1Descriptive Analysis (2019–2024)
Children’s Hospital 1, a major tertiary pediatric referral center in southern Vietnam, experienced considerable fluctuations in clinical service volumes and supply chain demands between 2019 and 2024. These shifts were shaped by both pandemic-related disruptions and post-pandemic recovery surges, creating substantial strain on operational resources.
3.1.1Hospital activity
As shown in Table 2 and Figure 2, outpatient visits and inpatient admissions declined sharply during 2020–2021, reaching their lowest levels in 2021, before rebounding rapidly from 2022 onward. By 2024, service volumes had largely returned to, or exceeded, pre-pandemic levels.
| Year | Outpatient Visits | Inpatient Admissions | Bed Occupancy Rate (%) | Avg Length of Stay (days) | Total Surgeries | Cardiac Surgery | Interventional Cardiology |
|---|---|---|---|---|---|---|---|
| 2019 | 1,836,500 | 95,000 | 116.56 | 6.20 | 18,606 | 450 | 639 |
| 2020 | 1,194,100 | 70,412 | 90.15 | 6.54 | 15,591 | 408 | 555 |
| 2021 | 556,056 | 37,951 | 50.13 | 6.75 | 10,573 | 358 | 456 |
| 2022 | 1,313,591 | 79,036 | 87.85 | 6.09 | 27,120 | 300 | 598 |
| 2023 | 1,347,168 | 89,705 | 102.50 | 6.26 | 31,154 | 476 | 810 |
| 2024 | 1,373,660 | 91,084 | 103.87 | 6.26 | 29,246 | 588 | 840 |
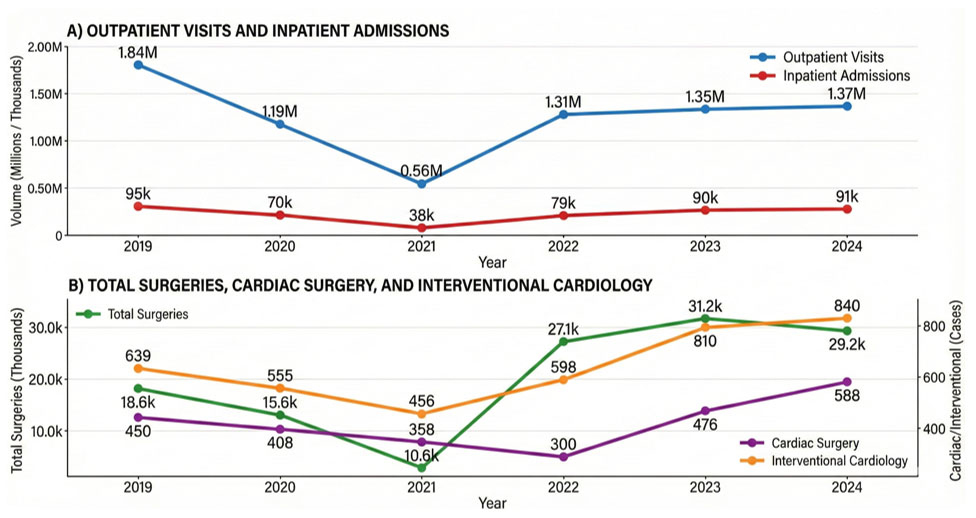
Figure 2.
Trends in clinical service volume and surgical complexity at Children’s Hospital 1 (2019–2024)
Despite this recovery, operational pressure remained high. Bed occupancy rates exceeded 100% in 2023–2024, indicating sustained capacity strain, while average length of stay remained relatively stable at approximately 6.26 days. Surgical activity followed a similar trajectory, with total procedures more than doubling between 2021 and 2023. High-complexity services, particularly cardiac surgery and interventional cardiology, increased steadily throughout the post-pandemic period.
These findings reflect not only service recovery but also a qualitative shift toward higher clinical intensity. This evolving demand profile provides critical context for assessing inventory performance and underscores the need for more responsive and risk-adaptive supply chain management.
The post-pandemic surge in high-complexity care placed increasing pressure on inventory coordination, particularly for specialty items, highlighting the limits of traditional bulk-based stocking policies.
3.1.2Integrated performance and operational stress metrics
The hospital’s inventory system exhibited persistent stress signals despite nominal improvements in lead times. As detailed in Table 3, the proportion of urgent procurement requests peaked at 34.7% in 2021 and remained elevated at 21.4% in 2024. Stock-out rates remained above 10% throughout the study period, indicating a fundamentally reactive system.
| Year | Service Level (%) | Stock-out Rate (%) | Days of Inventory | Urgent Requests (%) | Late Deliveries (%) | Expired Items (% value) |
|---|---|---|---|---|---|---|
| 2019 | 85 | 15 | 72 | 18.2 | 12.4 | 2.5 |
| 2020 | 86 | 14 | 70 | 22.0 | 14.1 | 3.0 |
| 2021 | 87 | 13 | 65 | 34.7 | 20.3 | 3.8 |
| 2022 | 88 | 12 | 62 | 30.5 | 17.2 | 3.1 |
| 2023 | 87 | 13 | 60 | 25.6 | 15.0 | 2.7 |
| 2024 | 88 | 12 | 58 | 21.4 | 13.3 | 2.2 |
3.2Inventory classification: ABC–XYZ matrix
To improve control over high-value medical inventories and support evidence-based decision-making, the hospital applied a dual-layer classification system combining the ABC and XYZ analytical methods. This framework was used to categorize all high-tech medical supplies managed between 2019 and 2024.
The ABC analysis ranked items by their annual consumption value. Class A items represented the top 10%–15% of items that consumed approximately 70%–80% of the total annual inventory budget. Class B and C items accounted for lower proportions of value but formed the majority in terms of item count. The XYZ analysis grouped items according to demand stability. Class X items showed regular, predictable usage; Class Y items had moderate fluctuations; and Class Z items displayed highly erratic or sporadic demand patterns. When combined, the ABC and XYZ classifications formed a risk–value matrix that enabled differentiated inventory policies for each item group. This segmentation facilitated more precise alignment between stocking strategies and consumption risk. Table 4 provides a cross-tabulation of inventory items by value (ABC) and demand variability (XYZ), revealing concentration patterns that inform risk-based stocking strategies and targeted JIT application. These bottlenecks span procurement processes, forecasting, inventory visibility, data integrity, and supplier performance, each contributing to cumulative inefficiency across the supply chain.
| X (Stable demand) | Y (Fluctuating demand) | Z (Irregular demand) | Total (%) | |
|---|---|---|---|---|
| A (High value) | 38.0% | 31.5% | 10.5% | 80.0% |
| B (Medium value) | 5.0% | 6.5% | 4.5% | 16.0% |
| C (Low value) | 1.0% | 1.5% | 1.5% | 4.0% |
| Total (%) | 44.0% | 39.5% | 16.5% | 100% |
3.3Performance gap analysis
Although moderate improvements were observed, the system continued to exhibit several persistent inefficiencies. An integrated review of performance indicators, internal audits, and stakeholder interviews revealed structural misalignments between inventory governance and clinical realities.
Key findings include:
- Procurement delays due to rigid multi-tier approval processes.
- Forecasting inaccuracies stemming from lack of integration with clinical workload data.
- Redundant stock accumulation caused by decentralized tracking and limited oversight.
- Expired stock and reordering errors driven by manual entry and inconsistent coding.
- Low supplier accountability leading to frequent delivery lapses.
Table 5 summarizes the key system-level bottlenecks identified through triangulated analysis of performance metrics, internal audits, and qualitative feedback from logistics and clinical stakeholders.
| Category | Issue Identified | Root Cause | Impact |
|---|---|---|---|
| Procurement workflow | Delays in purchasing approvals | Multi-level sign-off process | Prolonged lead time |
| Forecasting | Inaccurate order quantities | Lack of integration with clinical data | Overstock or urgent reorders |
| Storage & visibility | Redundant stocks across departments | Decentralized inventory tracking | High holding cost |
| Data management | Poor item-level traceability | Manual entry, inconsistent coding | Reordering delays, expired stock |
| Supplier performance | Unreliable delivery timelines | Weak contract monitoring | Increased late deliveries |
These systemic constraints limited inventory responsiveness and contributed to recurring operational inefficiencies, particularly during demand surges.
3.4Simulation results (2025)
A DES was conducted to assess the impact of transitioning to a JIT model. The simulation assumed real-time consumption tracking, recalibrated safety stocks, and VMI protocols for AX items, with procurement cycle time reduced to 15 working days.
Performance under the simulated JIT scenario demonstrated measurable efficiency gains (see Table 6 and Figure 3):
- Days of inventory decreased by 34.5%
- Stock-out rates declined by 45.8%
- Urgent procurement reduced by 57.0%
- Holding costs fell by 30.6%
- Service level improved modestly to 91.2%
| Performance Indicator | Baseline (2024) | Simulated JIT (2025) | % Change |
|---|---|---|---|
| Service Level (%) | 88.0 | 91.2 | +3.6 |
| Stock-out Rate (%) | 12.0 | 6.5 | –45.8 |
| Days of Inventory | 58 | 38 | –34.5 |
| Holding Cost (% of stock value) | 18.0 | 12.5 | –30.6 |
| Urgent Procurement Requests (%) | 21.4 | 9.2 | –57.0 |
| Procurement Cycle Time (days) | 30 | 15 | –50.0 |
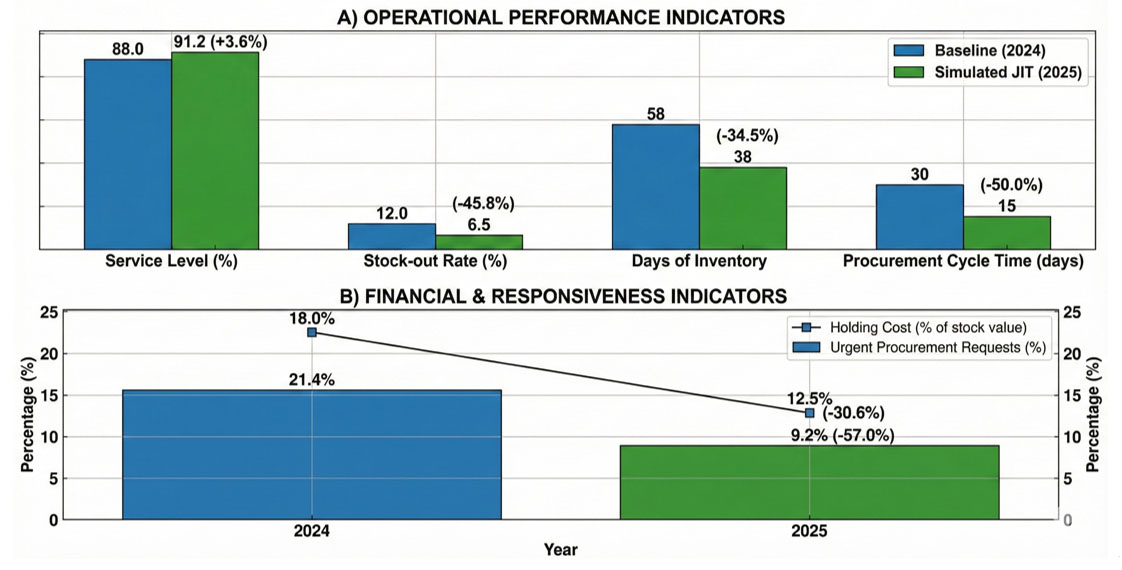
Figure 3.
Inventory performance outcomes: Baseline operations (2024) versus simulated JIT scenario (2025)
Sensitivity analyses showed that even under conservative assumptions, performance improvements were preserved—though to a lesser extent—highlighting institutional readiness as a prerequisite for scalability.
3.5Pilot validation (Q1/2025)
To validate simulation findings, a pilot JIT model was deployed in Q1/2025 in the Cardiovascular Intervention Department. The pilot included 42 high-priority items, mostly AX and AY class, and featured:
- Real-time demand capture from procedural logs
- Barcode-enabled tracking
- Automated reorder thresholds
- Vendor-managed replenishment
Operational results mirrored the simulation (see Table 7):
- Stock-out incidents: 72.7%
- Urgent procurements: 64.5%
- Inventory days: 35.3%
- Holding costs: 28.4%
- Zero procedure delays were reported during the pilot
| Performance Indicator | Q1/2024 | Q1/2025 (Pilot) | % Change |
|---|---|---|---|
| Stock-out Incidents (cases) | 11 | 3 | –72.7 |
| Urgent Procurement Requests | 31 | 11 | –64.5 |
| Average Days of Inventory | 51 | 33 | –35.3 |
| Holding Cost (% of stock value) | 17.5 | 12.5 | –28.4 |
| Procedure Delays due to Stock-outs | 2 | 0 | –100 |
Qualitative feedback emphasized reduced administrative burden, enhanced coordination, and increased staff confidence in inventory reliability.These findings confirm the feasibility of hybrid ABC–XYZ + JIT strategies under real-world constraints, provided adequate institutional support and supplier compliance.
4.Discussion
4.1Operational complexity and demand volatility
The longitudinal evidence from 2019 to 2024 demonstrates a widening structural gap between the evolving nature of clinical demand and the functional capacity of the hospital’s inventory system. At Children’s Hospital 1, demand volatility manifested not only in patient volumes but also in the acuity and supply intensity of care. While outpatient visits and inpatient admissions declined sharply during the COVID-19 period (2020–2021), the post-pandemic recovery phase was marked by a rapid rebound and subsequent overload, with bed occupancy rates exceeding 100% from 2023 onward and a substantial increase in high-complexity interventions.
In particular, interventional cardiology and surgical procedures more than doubled compared to 2021 levels, creating non-linear pressure on high-cost, short-shelf-life items.These dynamics exposed the limitations of an inventory system designed around historical averages, fixed reorder cycles, and bulk procurement logic. Although selected aggregate indicators—such as average length of stay or service level—appeared relatively stable, disaggregated analysis revealed persistent stress signals. Stock-out rates remained above 10% throughout the study period, urgent procurement peaked at 34.7% in 2021, and expired inventory approached 4% of total stock value, indicating a system that remained fundamentally reactive despite incremental improvements. Furthermore, internal audit logs indicated persistent mismatches between item consumption and ordering frequency in departments with fluctuating patient acuity, such as emergency and surgical units.
This apparent contradiction between stable macro-level indicators and deteriorating item-level performance echoes concerns raised by Ahmad et al.,[22] who cautioned that aggregated hospital metrics often mask operational fragility at the SKU or departmental level. In the present study, this masking effect translated into delayed replenishment of critical supplies during periods of clinical surge, while surplus inventory accumulated elsewhere, particularly among low-value but erratically consumed items. For example, during peak months of 2023, departments experienced simultaneous shortages of cardiac catheters and oversupply of low-use consumables like specific feeding kits, highlighting a lack of dynamic coordination.
Unlike earlier qualitative or cross-sectional studies that identified procurement rigidity as a general bottleneck,[23] the six-year dataset demonstrates how repeated episodes of unmodeled demand variability accumulate into systemic inefficiency.Attempts to expedite purchasing during high-demand periods were often slowed by rigid quarterly budgeting processes and lack of real-time inventory visibility, further compounding system stress.
In a pediatric tertiary context, these misalignments carry heightened risk. Short-term stock-outs of specialized devices or consumables can delay time-sensitive interventions, amplifying clinical consequences beyond financial inefficiency.
Collectively, the findings challenge the continued reliance on conventional inventory models that assume demand regularity and cost optimization through volume purchasing. Instead, they point to the necessity of inventory governance frameworks that explicitly recognize volatility as a core operational condition rather than an exception.[8,21,23] This includes embedding risk tolerance thresholds, proactive buffer mechanisms for high-acuity items, and digital synchronization between clinical service forecasts and supply chain decisions.
4.2ABC–XYZ classification as a risk-based decision framework
The implementation of the ABC–XYZ matrix in this study marked a significant transition from undifferentiated inventory control to a structured, risk-based governance model. By jointly stratifying inventory items based on annual consumption value (ABC) and demand variability (XYZ), the matrix unveiled nuanced consumption-risk patterns that would have remained obscured under one-dimensional approaches. This dual-layer stratification provided a granular understanding of item-level behavior, facilitating more precise risk prioritization and resource allocation. Empirical results revealed that Class A items—comprising approximately 80% of total inventory value but only a small fraction of SKUs—were predominantly classified as X or Y in variability. These items demonstrated stable or moderately fluctuating usage, suggesting strong suitability for tighter control, automated replenishment, and JIT-style protocols. Yet, in prior practice, they had often been managed under uniform policies alongside lower-priority items.[5,20] Conversely, CZ and BZ items, although low in financial impact, were disproportionately associated with demand unpredictability, stock expiry, and redundant intra-hospital distribution.[8,19,22] Analysis of expired stock reports from 2021–2023 confirmed that over 60% of expired items belonged to CZ and BZ categories, despite their low overall budget share.
Crucially, this reinforces the need to treat low-value/high-volatility items not as negligible but as high-risk categories for waste and inefficiency, particularly in budget-constrained LMIC settings. The value of the ABC–XYZ framework in this study lies not only in its analytical clarity but in its translation into operational policy. Specific procurement thresholds, review frequencies, and stock management strategies were tailored to each matrix segment. For example, AX and AY items were assigned continuous monitoring protocols with real-time alerts and automated restocking, while CZ items were excluded from bulk procurement cycles and managed via controlled, just-in-need requisition. This represents a significant advancement from prior literature, where ABC–XYZ matrices are often limited to descriptive analysis rather than integrated into procedural governance.[8,11,15] The hospital developed matrix-specific SOPs (Standard Operating Procedures), linking inventory review cadence and approval layers directly to classification category, thereby institutionalizing the framework into daily operations. However, a key limitation of the ABC–XYZ model is its omission of clinical criticality, perishability, and emergency-use frequency—factors crucial in high-acuity domains such as pediatric surgery and intensive care.
For instance, low-cost items like resuscitation drugs or antitoxins, though low on ABC, may carry life-or-death urgency. In future applications, the integration of multidimensional frameworks (e.g., ABC–VEN, criticality scoring) could enhance decision fidelity by aligning financial and operational risk dimensions with clinical importance.[8,10] Preliminary mapping exercises initiated in Q4/2024 have begun incorporating VEN tags and emergency-use flags to supplement ABC–XYZ stratification, indicating institutional readiness for multi-factorial classification. Ultimately, risk-informed stratification using ABC–XYZ created the structural foundation necessary for subsequent optimization strategies. Without clear differentiation between predictable and erratic demand, any attempt to implement lean or JIT models would risk either over-buffering or dangerously thin inventory levels.[5,12,19] By aligning classification with policy, the hospital was able to operationalize a responsive, tiered inventory governance approach suitable for the volatile demands of a tertiary pediatric institution.
4.3Simulating the Just-in-Time model: Projected impacts and constraints
Building upon the ABC–XYZ stratification, a DES model was developed to assess the operational feasibility and projected impact of transitioning to a JIT inventory strategy. Unlike idealized simulations, this model incorporated hospital-specific parameters, including historical consumption data, supplier performance variability, lead-time distributions, and procurement cycle governance. This ensured that the outputs were grounded in contextual realism rather than theoretical abstraction.The simulation was conducted using Arena software version 16.1, with sensitivity analyses performed on procurement lead time, demand fluctuation, and service-level targets to validate robustness of results.
The simulated results revealed considerable performance gains. Relative to the 2024 baseline, stock-out rates were projected to decline by 45.8%, average inventory days reduced by 34.5%, and urgent procurement requests decreased by over half. Holding costs dropped by approximately 30%, and service levels showed a modest increase.These improvements suggest not only increased efficiency but also enhanced system responsiveness under constrained resource settings. However, these improvements were not evenly distributed across item classes. AX-class items—those with high financial value and stable demand—performed exceptionally well under JIT conditions,[12,15] with reduced stock volatility and predictable replenishment cycles.
In contrast, items categorized as BZ or CZ—characterized by low value but high variability—remained vulnerable to disruptions. The simulation emphasized that for these classes, JIT must be complemented by auxiliary strategies, such as buffer stock reserves, consignment models, or multi-source contracts.[5,8] Notably, BZ items showed a simulated increase in stock-out events when modeled under full JIT without safety stock buffers, reaffirming the importance of differentiated policy application. A critical modeling assumption involved reducing the procurement cycle time from 30 to 15 days-an improvement that hinges on broader system reforms, including enhanced digital integration, streamlined approval hierarchies, and supplier performance accountability. This highlights that the success of JIT is not merely a matter of inventory mathematics but is contingent on structural and governance transformation.[13,18,21,23]
During scenario testing, the model demonstrated that without at least a 30% reduction in cycle time, service level gains plateaued and urgent orders remained above 15%, reinforcing the dependency on institutional reform. To validate the model and manage risk, the pilot implementation deliberately focused on AX and AY items, which inherently carry lower operational uncertainty. This targeted selection aligns with risk management best practices,[7,8,9] but it also introduces an element of selection bias. The findings should therefore be interpreted as proof-of-concept for phased application, beginning with predictable items and gradually expanding toward more complex and variable categories. Moreover, the simulation did not incorporate labor availability constraints, which may influence real-world responsiveness during scale-up. Future modeling iterations should consider workforce dynamics, warehousing limitations, and supplier behavior in stressed contexts.
4.4Real-world validation: Evidence from the cardiovascular supply pilot
The Q1/2025 pilot implementation in interventional cardiovascular supplies provided critical real-world validation of the simulation findings. By focusing on a high-risk, high-value category dominated by AX and AY items, the pilot tested JIT principles under operational conditions rather than theoretical assumptions.The pilot selection process used a multi-criteria prioritization tool that considered historical demand stability, stock-out frequency, and financial value to identify suitable items for initial JIT rollout. The observed improvements were substantial. Stock-out incidents declined by 72.7%, urgent procurement requests by 64.5%, and average days of inventory by over 35%, while holding costs decreased by nearly 30%. Importantly, no procedures were delayed due to supply unavailability during the pilot period. These results underscore not only quantitative performance gains but also a high degree of implementation feasibility within constrained environments.
Additionally, cycle time for procurement approvals within the pilot department was reduced by 40%, largely due to delegation of authority and digitized requisition workflows. Beyond quantitative gains, qualitative feedback from clinicians and logistics staff highlighted improved predictability, reduced administrative burden, and greater confidence in the supply system.[8,11,17] These behavioral dimensions are critical, as trust in inventory reliability often determines whether clinical teams adhere to formal procurement pathways or resort to informal workarounds. Interviews with clinical leads indicated that improved visibility into item availability through integrated dashboards reduced pre-procedure uncertainty and eliminated informal stock hoarding practices.Such behavioral shifts are essential enablers of system transformation, but often overlooked in quantitative evaluations.
At the same time, the pilot revealed practical nuances. Certain items required micro-buffering due to clustering of procedures, and supplier performance variability necessitated closer monitoring. These observations informed the refinement of a hybrid model, blending JIT with selective redundancy—a pragmatic adjustment that enhances resilience without reverting to blanket overstocking.[19,24] As a result, the hospital developed a contingency protocol defining buffer thresholds for procedure-linked items based on historical clustering data, reviewed quarterly.
4.5System-level constraints and strategic implications
Despite the encouraging results observed in both the simulation and pilot phases, the transition toward full-scale implementation of a hybrid inventory management model remains constrained by persistent system-level barriers. These constraints extend beyond technical limitations and are deeply embedded within institutional structures, governance arrangements, and organizational norms that shape procurement and logistics practices. A primary obstacle lies in procurement rigidity. Fixed quarterly budgeting cycles and multi-tiered approval processes continue to restrict the hospital’s ability to respond dynamically to fluctuations in clinical demand.[22,24] Such procedural inflexibility prolongs replenishment lead times and weakens alignment between inventory decisions and real-time service requirements. Even when analytical tools indicate imminent shortages or excesses, corrective action is often delayed by administrative procedures. This structural lag undermines the potential efficiency gains projected under JIT scenarios. Equally consequential is the fragmentation of information systems. Persistent data silos between inventory management, procurement units, and clinical departments limit visibility across the supply chain and compromise forecasting accuracy.[13,17,22] In practice, procurement decisions are frequently based on partial or outdated data, reinforcing reactive purchasing behaviors and increasing reliance on urgent procurement. Supplier performance management represents a further systemic vulnerability. The absence of formalized monitoring mechanisms, performance benchmarking, and enforceable accountability frameworks allows external variability—such as delayed deliveries or incomplete order fulfillment—to propagate unchecked into internal operations. Such instability poses particular risks for JIT-based systems, which rely fundamentally on predictable and reliable supply streams.[1,18,25] Organizational culture also exerts a powerful influence. Long-standing reliance on buffer stock—while sometimes operationally necessary—reflects not only logistical risk mitigation but also institutional memory shaped by prior supply failures. Over time, this experience fosters risk-averse procurement norms, in which lean approaches such as JIT are perceived as unsafe or impractical.
Although the pilot intervention contributed to rebuilding confidence in tighter inventory cycles, scaling such reforms will require deliberate and sustained change management. Importantly, the findings do not support the wholesale replacement of conventional inventory models with JIT. Rather, they point toward the value of a strategically hybrid approach. JIT principles appear most appropriate for items that combine high clinical criticality with relatively stable demand profiles, while buffers or redundancy remain necessary for items characterized by high variability or supplier uncertainty.[3,8,14,26] Such selective integration allows hospitals to balance efficiency gains with resilience.
In pediatric tertiary care settings, the consequences of inventory failure are particularly severe. Clinical areas such as interventional cardiology or intensive care demand near-absolute supply reliability, as even short-term stock-outs may delay life-saving interventions. In this study, these risks were mitigated through embedded safeguards, including micro-buffering of time-sensitive items, integration of procedural logs with real-time inventory dashboards, and predefined fallback protocols for supplier non-fulfillment. While these measures enabled efficiency improvements without compromising patient safety, their sustainability depends on disciplined execution, continuous performance monitoring, and clearly defined cross-functional accountability.[2,16,20] Ultimately, the hybrid inventory governance model advanced in this study offers a pragmatic pathway for reform in LMIC hospital systems—balancing cost-efficiency with clinical responsiveness under real-world institutional constraints.
5.Conclusion
This study demonstrates that a hybrid, risk-based inventory strategy—combining ABC–XYZ classification, JIT principles, and simulation-driven validation—can improve both operational efficiency and clinical service reliability in a pediatric tertiary hospital. Beyond technical gains, the intervention offers strategic insights into how inventory systems can be governed more dynamically, with differentiated policies tailored to risk profiles and demand patterns.
The findings offer practical and strategic implications for hospital leaders seeking to modernize supply chain management within complex, resource-constrained environments. The success of the hybrid inventory model was not merely a function of algorithmic optimization, but the result of deliberate institutional alignment and administrative stewardship.
From a policy perspective, the transition away from uniform, buffer-heavy inventory practices requires a shift toward differentiated governance models. This involves enabling flexible procurement cycles, integrating real-time data flows, and revising approval hierarchies to reduce decision latency. Hospital policy must also address supplier accountability and ensure contractual mechanisms support responsive fulfillment—core preconditions for JIT success.
These findings are especially relevant for tertiary pediatric hospitals, where volatility in demand and clinical urgency amplify the operational risks of inventory failure.
On the administrative front, leadership plays a critical role in change management. Resistance to lean practices is often rooted in legacy risk-avoidance behaviors, especially in systems that have experienced prior supply failures. Building trust in dynamic replenishment models requires not only pilot validation but also consistent communication, stakeholder engagement, and clear governance protocols. Cross-functional collaboration between clinical, financial, and logistics departments must be formalized, with shared accountability for inventory performance. As shown in the pilot implementation for cardiovascular supplies, even small-scale success can act as a proof of concept to drive cultural and procedural change.
This model also highlights the importance of capacity building in health systems. For LMIC hospitals, inventory transformation is inextricably linked to broader goals such as digital health integration, institutional resilience, and fiscal sustainability. Policymakers and administrators should view inventory reform not as a narrow operational fix, but as a strategic lever to enhance system performance, reduce waste, and improve care continuity.Future applications should prioritize phased implementation and incorporate safeguards such as risk-based item selection, micro-buffering, and contingency protocols.
Rather than advocating for wholesale replacement, this research proposes an adaptive inventory governance framework where JIT is deployed selectively—under administrative oversight and with safeguards—to balance responsiveness, safety, and cost-effectiveness. For hospital administrators seeking to modernize supply chain systems, this model provides a context-anchored roadmap rooted in both evidence and practical implementation.
Ultimately, this study positions inventory policy not just as a technical issue, but as a strategic governance challenge—one that demands deliberate policy shifts, adaptive leadership, and systems thinking at every level of hospital administration. In doing so, it contributes to a growing body of evidence that inventory reform, when aligned with institutional realities, can be a powerful driver of health system performance in LMICs.
Authors contributions
Tam Trung Phan Duong conceptualized the study, conducted the primary analysis, and drafted the manuscript. Nguyen Dinh Pham supervised the project, contributed to methodological refinement, and reviewed all manuscript versions. Both authors contributed to the interpretation of results and approved the final manuscript for submission.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of Interest Disclosure
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
The requirement for individual informed consent was waived due to the retrospective nature of the study and the use of anonymized administrative data.
Ethical statement
The study protocol was approved by the Institutional Review Board of Children’s Hospital 1, Ho Chi Minh City. All procedures were conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Ethics approval
The Publication Ethics Committee of the Association for Health Sciences and Education. The journal’s policies adhere to the Core Practices established by the Committee on Publication Ethics (COPE).
Provenance and peer review
Not commissioned; externally double-blind peer reviewed.
Data availability statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Data sharing statement
No additional data are available beyond those described in the manuscript.
Acknowledgements
We express our sincere gratitude to the Board of Directors of Children’s Hospital 1 for their institutional support and for facilitating the data access essential to this research. We are deeply grateful to the personnel of the Equipment and Medical Supplies Department and the Cardiology Department for their vital cooperation during the data collection and the Just-in-Time pilot implementation phases. Special thanks are also extended to the clinical and administrative stakeholders whose professional insights were fundamental in identifying systemic bottlenecks and refining the discrete-event simulation model.
References
- World Health Organization. WHO procurement report 2022. 2022.
- The Lancet Global Health Commission. Financing primary health care: putting people at the centre. Lancet Glob Health. 2022;10:e715-e772. doi:10.1016/S2214-109X(22)00005-5
- Ngo L, Tran-Thi H, Dang T. Analysis of drug inventory characteristics in 2022 and establishment of safe stock levels for 2023 at Thong Nhat Hospital, Ho Chi Minh City. Ho Chi Minh City Journal of Medicine. 2024;27(1):29-37.
- Nguyen T, Tran V, Pham T. A study on establishing drug inventory norms using the EOQ model at the main warehouse of Kien Giang General Hospital from 2020 to 2022. Can Tho University of Medicine and Pharmacy Journal. 2023;66:1-7.
- Venkatesh P, Sowmiya P. ABC-XYZ Classification and Forecasting for Inventory Optimization. International Journal of Research Publication and Reviews. 2024;5(12):5348-5357. doi:10.55248/gengpi.5.1224.0227
- Nguyen P, Dang T, Nguyen T. 5-year inventory management of drug products using ABC-VEN analysis in the pharmacy store of a specialized public hospital in Vietnam. Pharmacia. 2022;69:517-25. doi:10.3897/pharmacia.69.e84348
- Singh S, Sharma H, Aggarwal V. ABC and XYZ analysis in the medical store of a government tertiary care cancer hospital of North India. Indian J Pharm Pract. 2026;19(2):232-9. doi:10.5530/ijopp.20260539
- Assis A, Santos A, Santos L. Classification of materials and medicines in hospital inventory management: a multi-criteria analysis . Res Sq. 2022. doi:10.21203/rs.3.rs-1709110/v1
- Herlambang C, Parung J. Information system design and inventory management on pharmacy business within ABC-XYZ analysis method. Airlangga J Innov Manag. 2021;2(2):194-205. doi:10.20473/ajim.v2i2.31124
- Kaur B, Garg N, Gad V. A study to carry out always better control and vital, essential, and desirable analysis in the dispensary of a tertiary care teaching hospital. J Mar Med Soc. 2023;25(2):150-3. doi:10.4103/jmms.jmms_183_22
- Delgado S, Lopez-Herrera Y, Castro P. PDCA model for increasing the inventory turnover rate through integration of ABC, 5S, Kanban and cycle counting in a Peruvian pharmaceutical SME. Proc Int Conf Ind Eng Oper Manag. 2023:198-205. doi:10.1145/3629378.3629392
- Martin D, Fernández C, Gento Municio Á. Systematic review of discrete event simulation in healthcare and statistics distributions. Appl Sci. 2025;15(4):1861. doi:10.3390/app15041861
- Musliadin A, Apriadi D. Optimizing hospital pharmaceutical warehouse operations using discrete event simulation. J Riset Ilmu Tek. 2024;2(2):100-116. doi:10.59976/jurit.v2i2.97
- Veres P. Increasing the efficiency of warehouse analysis using artificial intelligence. Acta Logistica. 2023;10(3):445-51. doi:10.22306/al.v10i3.415
- Gomaa A. Improving supply chain management using Lean Six Sigma: a case study. Int J Appl Phys Sci. 2023;9(1):9-25. doi:10.20469/ijaps.9.50002
- Freeman-Muhammad S, Chipman-Ashley R, Martin R. Impact of connected dispensing technology with advanced analytics in a multicenter health system. Am J Health Syst Pharm. 2024;81(23):e760-e769. doi:10.1093/ajhp/zxae198
- Tanzubil B. Effect of logistics management practices on medical diagnostic efficiency in public hospital facilities in Ghana. Afr J Appl Res. 2025;11(5):148-72. doi:10.26437/r5fckw20
- Lawrence S, Mupa M. Supply chain tools and its central importance to distribution chain efficiency in West Africa: Nigeria and Ghana as case studies. Afr J Logist Supply Chain. 2024;8:286-307.
- Zhu Q. Multi-echelon inventory optimization framework with ABC-XYZ classification: evidence from simulation-based validation [Internet]. 2025. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=5407306
- Chuang Y, Hu J. Comparative assessment of health systems resilience: a cross-country analysis using key performance indicators. Systems. 2025;13(8):663. doi:10.3390/systems13080663
- World B. Global Supply Chain Disruptions: Competition Policy Implications. Equitable Growth, Finance & Institutions Notes; Equitable Growth, Finance & Institutions Insight; Trade, Investment and Competitiveness. © World Bank. 2022. License: CC BY 3.0 IGO http://hdl.handle.net/10986/37507
- Demiray Kırmızı S, Ceylan Z, Bulkan S. Enhancing inventory management through safety-stock strategies-A case study. Systems. 2024;12(7):260. doi:10.3390/systems12070260
- Manivannan P, Mehta C, Thomas S. Improving supply chain management of medicines for public healthcare in India. 2024. Working Papers 36, xKDR
- Tran T, Hoang T. Improve supply chain management capacity at the public hospital under the Ministry of Health in Hanoi. Int J Adv Multidiscip Res Stud. 2024;4(3):64-68.
- Masemola S, Omoruyi O, van der Westhuizen J. Antecedent factors of procurement performance in the public health sector in the Gauteng Province. Afr J Inter/Multidiscip Stud. 2022;4(1):250-63. doi:10.51415/ajims.v4i1.983
- Mashayekhy Y, Babaei A, Yuan X. Impact of Internet of Things (IoT) on inventory management: a literature survey. Logistics. 2022;6(2):33. doi:10.3390/logistics6020033
 This work is licensed under a
This work is licensed under a 